

Chapter 3 - Apandemia - Part 5
By Stefano Scoglio - translated to English from Italian

This is the final part of Chapter 3. I am so excited to move on to Chapter 4.
It is difficult for me to gauge interest in this translation of the book Apandemia by Stefano Scoglio. How would I know if people like it or are interested? We all should know by now that the internet is not free. Since I cannot reasonably assume that people are interested in this book, I have made a separate section for the book, this way you can unsubscribe to future notifications, specific to this book. I have made a post that explains how you can subscribe only to the book or only to my other posts. Here is that post:

THE ROLE OF EARLIER FLU VACCINES IN THE “SECOND WAVE”
But there is another even more plausible explanation for the 2020 mortality increase. It is necessary to distinguish between the alleged first wave and second wave, terms we accept to discuss despite even “epidemiologists not being sure it is useful to conceptualize pandemics as structured in waves.”🦶1 32

In my first analysis of ISTAT’s COVID-19 statistics, I noted that even during the initial March–April phase, only a minority of reported cases could clearly be attributed to COVID-19 itself—and that many of those severe outcomes may have been linked more to aggressive intubation protocols than to contagion. I also cautioned against overlooking the possible impact of mass vaccination campaigns. The two areas most affected by the alleged pandemic, Bergamo and Brescia, had carried out extensive vaccination drives in the preceding months: around 185,000 flu shots and approximately 80,000 meningococcal vaccinations, often administered concurrently, creating potentially harmful interactions. I further referenced an article published in Avvenire, where local physicians reported several cases of fatal pneumonia occurring even before the COVID narrative emerged, remarking with surprise that “they were all vaccinated.”🦶2 33
An unusual and highly significant fact is connected to the sharp rise in deaths observed in October and especially November: the earlier start of the flu vaccination campaign. As the Ministry of Health reported, “Data on flu vaccination for the 2019/2020 season show, in the general population, an increase in coverage from 15.8% of the previous season to 16.8% of the last season. In the elderly especially, starting from the 2015/16 season, a constant increase in coverage is observed, settling at 54.6%.”
Since flu vaccinations are mainly administered to people over 65, a 1% increase in national vaccination coverage likely corresponds to at least a 5% rise among this age group—a group that, in 2019, already accounted for more than half of all vaccinated individuals, in a steadily growing trend. This year, coincidentally, the vaccination campaign—which usually starts gradually in mid-October, intensifies in November, and peaks in December—was moved up to begin on October 1 and began at full speed, justified by the stated need to better distinguish cases of flu from COVID.
Flu Vaccination
When to get vaccinated
This year, given the current epidemiological situation regarding the circulation of SARS-CoV-2, it is recommended to advance flu vaccination campaigns starting from early October and offer vaccination to eligible individuals at any time during the flu season, even if they show up late for vaccination. This can be particularly important if it is a late flu season or when high-risk patients present. The decision to vaccinate should take into account the incidence level of flu-like syndrome in the community, keeping in mind that the immune response to vaccination takes about two weeks to fully develop.
Publication date: December 12, 2016, last update September 10, 2020
Along with the earlier start of the vaccination season, flu shots were made free for the first time to those over 60, instead of only those over 65. The move was accompanied by an intensive media campaign urging people to get vaccinated, supposedly to help doctors and hospitals better distinguish true COVID cases. The logic behind this argument was that if someone vaccinated against influenza later developed flu-like symptoms, it could only be COVID.
Coincidentally or not, the sharp rise in deaths during October and November paralleled the progressive rollout of mass flu vaccination among the elderly. I recently published an article discussing the potential cardiovascular risks of flu vaccines, which contain unspecified amounts of potassium chloride and phosphate—substances that may pose added risks to frail or elderly individuals. This topic will be explored in more depth in the chapter devoted to vaccines. There, we will also examine how COVID vaccines appear to be even less effective and more harmful than flu vaccines, potentially contributing to a further rise in mortality in the coming months—figures that may, once again, be attributed to the so-called “pseudo-pandemic.”
The Impact of 5G
As we will see, although overall mortality rates remained well within the normal range—indicating that no true pandemic occurred—the pattern of pneumonias observed this year shows certain peculiarities that may be linked to the introduction of 5G networks. Indeed, 2020 marked the year of large-scale 5G deployment:
“We are almost there: after so many announcements and long waiting, 2020 is the year when 5G networks will become available to everyone, or almost... Almost all Italian mobile operators activated the first 5G repeaters last summer (Summer 2019 - NdR) and plan to greatly expand coverage throughout 2020. TIM, for example, started with Rome, Turin, and Naples (university citadel), then moving to Milan, Verona, Florence, Matera, and Bari...”🦶34 3
It is not yet possible to make comparative evaluations between 5G rollout and increases in pathologies, especially because there are no transparent data on 5G presence in the territory. But it is a line of research to keep in mind, because as we saw, there is no doubt that the areas most hit by the pseudo-pandemic, Wuhan as well as Bergamo, besides being spearheads of mass vaccinations, were also avant-gardes for the installation of 5G antennas.
Before evaluating in more detail the aforementioned toxemic factors, we conclude this chapter with the analysis of the latest ISTAT reports on the increase in deaths throughout 2020.
ISTAT TALKS OF 100,000 MORE DEATHS IN 2020. BUT WHAT DID THEY DIE OF?
Il Miglioverde, March 11, 2021
ISTAT has just released its latest—fifth—report on 2020 mortality,🦶354, stating that there were 746,146 deaths last year, an increase of 100,526 compared to the 2015–2019 average, or +15.6%. The media and pandemic enthusiasts greeted the news with almost celebratory enthusiasm, as if it finally provided proof—against all “deniers”—that yes, there was indeed something resembling a pandemic. Not much of one, perhaps, but, as they would say, details…
I will not dwell on the details of this latest Report, which largely reiterates the themes and data already presented in earlier editions and that I have discussed extensively in previous writings. Instead, I will focus on a few key points. First: why do all media outlets insist on speaking of 100,000 COVID deaths, when the report itself explicitly states that there were 100,500 more deaths than the previous five-year average, and, at the same time, attributes 75,000 of these to COVID? Even in the most favorable interpretation (for them), the pandemic could have accounted for at most 75,000 excess deaths. But where is the proof that these 75,000 COVID deaths are actually included within the 100,000 total excess deaths? As in previous reports, this one too is clearly constructed with a propagandistic intent—to assert that the mortality increase is both unprecedented and directly attributable to the COVID-19 pandemic. All accompanying graphs, including the one below, are designed to emphasize how the rise in deaths neatly overlaps with the so-called “pandemic waves.”
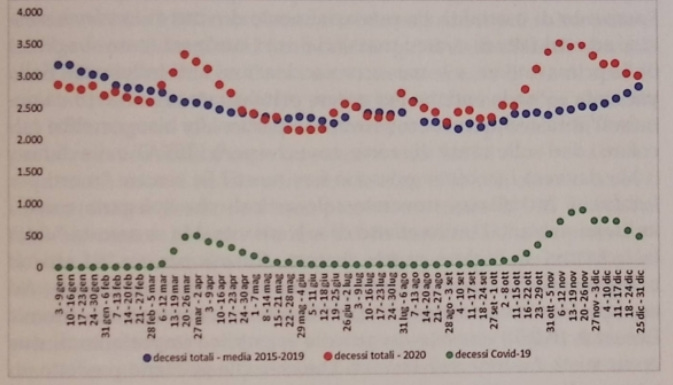
This graph refers to Central Italy, and it is unclear why ISTAT chose not to present a single graph for the entire country, opting instead for three separate ones corresponding to the North, Center, and South. Perhaps the reason is that including the South would have lowered the overall average, making the visual impact less dramatic. As is well known, statistics can be shaped to support particular narratives, and in this case, it seems evident that the intention is to suggest a correlation between mortality surges and the rise in deaths attributed to COVID.
Even at this stage, the first inconsistencies become apparent: the peaks in mortality align not only with increases in deaths involving COVID but also with the periods of lockdown. Notably, the red dots representing excess mortality rise sharply around March 10—the start of the first lockdown—and remain elevated until the end of April, precisely matching the duration of that confinement. Similarly, the so‑called second wave, which began in mid to late October and lasted through December, coincides with the second lockdown introduced by the Conte government beginning on November 4.
Admittedly, data can be interpreted in many ways. Supporters of the dominant pandemic narrative may argue that lockdowns helped prevent the further spread of the virus. However, one might also consider that the rise in mortality could stem from the lockdowns themselves or from other contributing factors—such as the widespread iatrogenic errors (mistaken treatments) during the first wave, and the mass influenza vaccinations preceding the so‑called second wave. To privilege one interpretation over another, solid evidence is required—particularly detailed data on causes of death, which ISTAT has conspicuously avoided producing.
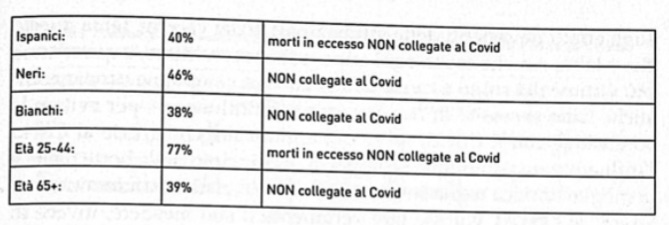
But can lockdowns actually cause deaths? If you search “morti per lockdown” in Italian, you’ll find only articles insisting that lockdowns serve exclusively to save lives. Yet, if you search “death by lockdown” in English, you can access—at least for now—studies and discussions that are completely silenced in what has become the Italian information lockdown. For instance, the American Institute for Economic Research (AIER) cites an important study by economists Audrey and Thomas Duncan, who predicted an excess mortality of no fewer than 100,000 deaths attributable to lockdown measures. As AIER points out, despite its sound scientific basis, this research was entirely ignored by mainstream media. The article also draws on official CDC (Centers for Disease Control and Prevention) data, revealing a dramatic increase in deaths unrelated to COVID.🦶365:
These figures align with the data I first highlighted in my initial analysis of ISTAT records. In Bergamo, for instance, between February 20 and March 31, 2020, there were 6,238 total deaths—compared with an average of 1,180 deaths during the same period over the previous five years. Of these, only 2,346 were classified as deaths with COVID, leaving 3,892 deaths from other causes. In other words, while deaths involving COVID (setting aside the official report that 95% of these cases involved individuals over 80 with multiple serious preexisting conditions) represented a 100% increase over the historical average, deaths from other causes soared by an astonishing 333%.
The same pattern was seen in other cities with high excess mortality. In Pesaro, for instance, there were 912 total deaths between February and March, compared with an average of 454 during the same period over the previous five years. Of these, only 157 were attributed to COVID, leaving 755 deaths from other causes. 🦶376 In other words, deaths with COVID accounted for just 34% of the five‑year average, while deaths from other causes amounted to 166% of that average. Isn’t it time we tried to understand what the vast majority of these excess deaths were actually due to?
As I suggested in a previous paper, this large excess of “non‑COVID” deaths may be explained by a combination of factors: the effects of lockdowns (including depression, substance abuse, and isolation of untreated patients), inappropriate medical interventions (which persisted even after widespread acknowledgment of the harmful consequences of intubation), and vaccines — a taboo topic that nevertheless accounts for numerous casualties every year. This year, the toll may have been even higher due to aggressive campaigns urging flu vaccination to “avoid confusion” with COVID, only for the narrative to shift later, claiming that COVID had conveniently made the flu disappear. In pandemic journalism, it seems the principle of wanting both a full barrel and a drunk wife reigns supreme.
If ISTAT truly wished to fulfill its institutional role, rather than acting as a propaganda vehicle, it would have done the one thing capable of demonstrating COVID’s real contribution to excess mortality: analyzing and publishing data on the incidence of different causes of death — something it has carefully avoided. The institute also neglects another striking aspect: the anomalies in mortality by age group. Here is how ISTAT itself reports the situation of excess mortality across age brackets:

The first striking fact is that in 2020, mortality among those aged 0–50 actually decreased by 8.5% compared with the average of the previous five years. This figure alone should be enough to cast serious doubt on the very notion of a pandemic: how can a pandemic lead to a notable reduction in mortality for half of the population?🦶387 It would have to be a strangely benevolent pandemic — one that, for the most active and working segment of society, turned out to be a gift of longevity
But it is interesting to compare the above datum with COVID’s contribution to general mortality for each age class:
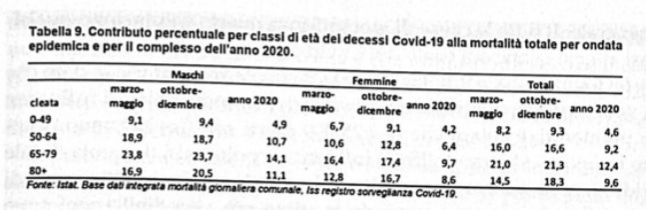
The comparison is significant because, if COVID deaths fully accounted for the rise in overall mortality, the increase in total deaths should correspond exactly to the number of COVID deaths. The age group most affected by the overall increase is, unsurprisingly, those over 80. According to ISTAT, this group accounts for 76.3% of total excess mortality — an increase of 76,708 deaths compared to the 2015–2019 average — which means the surge in deaths occurred primarily within this age bracket. ISTAT also reports that deaths among the over‑80s rose by 18.7%, bringing the total to 486,255 deaths. Since COVID deaths represent 9.6% of this total, that corresponds to approximately 46,680 deaths with COVID. This tells us something crucial: among the over‑80s, there are 30,028 excess deaths (76,708 − 46,680) not attributed to COVID. Subtracting these from COVID’s contribution to excess mortality reduces the total from 100,526 to 70,498.
This clearly shows that even the figure of 75,000 deaths “with COVID” does not fully account for the 100,000 excess deaths. Therefore, the claim that all 100,000 additional deaths were caused by COVID does not hold up. As noted, the only way to determine with certainty how many of these excess deaths were truly due to COVID — and how many to other causes — would be to assess the contribution of each cause of death to overall mortality. Without such an analysis, any assertion about COVID’s share in excess mortality remains pure propaganda.
COVID-19 is primarily a respiratory disease, and its symptoms largely overlap with those of common flu and pneumonia. If the 75,000 recorded deaths “with COVID” coincided with a decrease in flu and pneumonia mortality, that reduction should logically be subtracted from COVID’s contribution to excess deaths. According to the most reliable estimates, roughly 30,000 people die each year from influenza, mostly among those over 80. If flu mortality dropped by, say, 25,000 cases during the COVID period, then those 25,000 deaths were not additional but effectively replaced what would have been flu-related deaths. Since we have already discounted about 5,000 cases from the initial 75,000 COVID-related deaths when estimating the 100,000 total excess deaths, deducting an additional 25,000 would reduce COVID’s net contribution to about 45,000 deaths. This means that over half of the excess mortality would need to be attributed to causes other than COVID.
That this hypothesis may not be numerically exact yet still reflects reality is effectively acknowledged by ISTAT itself—albeit through a widely circulated and unconvincing justification:
“In January 2021, the absolute number of COVID-19 deaths reported by Surveillance exceeds the calculated excess mortality compared to the average of previous years. This phenomenon is likely attributable to a reduction in deaths from causes other than COVID-19, such as influenza, which—thanks to distancing measures—had a much lower incidence compared to 2015–2019.”
This explanation for the disappearance of influenza is difficult to reconcile with the assumption—central to virological theory—that influenza viruses and SARS-CoV-2 share similar modes of transmission. It remains unclear why masks and distancing would suppress the former while coinciding with a surge in the latter.
A more straightforward interpretation is that many deaths previously attributed to influenza or pneumonia were reclassified as COVID-19. ISTAT’s own data for January 2021 appear consistent with this view.
In that month, ISTAT reports approximately 70,583 deaths—about 2,000 above the five-year average, yet more than 5,000 fewer than the 75,623 recorded in January 2017. Of these, 12,527 were attributed to COVID-19. In the absence of a substantial increase in overall mortality, these COVID-19 deaths correspond to a comparable reduction in deaths from other causes, most likely influenza and pneumonia, the former having reportedly undergone a “sharp decrease.”
Therefore, by ISTAT’s own admission, deaths “with COVID” in 2020 did not necessarily add to overall excess mortality but largely replaced deaths from other causes, as observed in January 2021. This implies that the roughly 100,000 excess deaths—absent evidence to the contrary—must be attributed, at least in substantial part, to factors other than COVID-19.
We have already noted how a significant share of the approximately 30,000 annual influenza deaths appears to have been reclassified as COVID-19, reducing the number of cases plausibly contributing to excess mortality to around 45,000. Applying the same reasoning to pneumonia—which accounts for roughly 70,000 deaths each year—suggests that the January 2021 pattern may extend to 2020 as a whole.
Cause-specific mortality data are not yet available, so this conclusion cannot be stated with certainty. However, the available indicators point in this direction, and even ISTAT has not definitively quantified COVID-19’s contribution to excess mortality. What remains clear is the January 2021 figure: COVID-19 accounted for about 17% of total deaths without producing a corresponding increase in overall mortality.
Since the only major novelties in 2020 were COVID-19 and the lockdown measures, if the increase in deaths cannot be attributed to COVID-19, it must be sought elsewhere—namely in the effects of the lockdowns themselves. These include delayed, inadequate, or foregone medical care, increased vaccination campaigns, and a range of well-documented social and health consequences such as depression, suicide, substance abuse, and poverty-related malnutrition.
FOOTNOTES 🦶
35https://www.iss.it/18f52493-6076-9ec3-7eb2-b39efed8b22f Interesting to note how ISTAT has removed the document from its site, which is now only found on the Istituto Superiore di Sanità site.
36 Tucker J., Death by Lockdown, AIER, November 2, 2020. Death by Lockdown - AIER
37 Rapporto ISTAT su mortalità ai tempi del Covid.pdf
38 Popolazione per età, sesso e stato civile 2019 - Italia (tuttitalia.it)
''COVID’s share in excess mortality remains pure propaganda.''
1 of many examples below from the worlds only official COVID inquiries to reveal the truth to the lockdown in UK. Facts jettisoned throughout all media and prominent covid critic channels.
''People living with dementia died during the pandemic, not from COVID-19, but their lives were shortened because they did not understand what was going on and they gave up.’’
https://biologyphenom.substack.com/p/newscottish-covid-19-inquiry16-dec?utm_source=publication-search
Below is Scottish Government assumption-Feb 2022
''The number of deaths involving dementia that also had COVID-19 mentioned on the death certificate represented 99% of the number of excess deaths involving dementia. This supports our ASSUMPTION that excess deaths registered involving dementia in 2020 (2,177) could almost wholly be attributed to COVID-19.’’