

Chapter 3 - Apandemia - Part 4
By Stefano Scoglio - translated to English from Italian

note from Renee : I'm excited to dive into Chapter 4. Chapter 3 has been long. There's still Part 5 coming. This book is jam-packed with important information that we must not let be memory-holed.
MUCH ADO ABOUT NOTHING:
THE NEGLIGIBLE NUMBER OF COVID-19 DEATHS
The media hammering on the alleged COVID disasters continues: the other day, August 16, 2020, I watched TG1, just to see how far the propaganda had gone, and in half an hour of news, the first 15 minutes were completely dedicated to COVID-19! And one of the numbers used daily as a tool of outright psychological terrorism is the number of COVID-19 deaths worldwide: over 750,000! A number thrown out as if it were extraordinary, unprecedented…
Today, September 12, 2020, the number has risen to over 900,000:
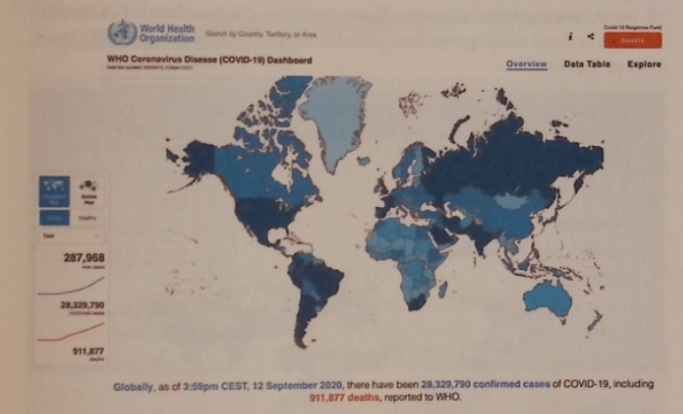
In reality, as we have seen, many of these COVID-19 deaths are mostly deaths from other causes “with” COVID (positive on the fake swab), and even deaths from other causes then passed off as COVID without even a positive swab. But let’s pretend they are real numbers: 911,000 deaths in 7 months. How many might there be in a year? The trend in deaths, after a peak in March, declined worldwide in June-September, and at the time I predicted about 1.5 million deaths attributed to COVID in a year.
In reality, since in October-November, as we will see, there will be a rise in mortality (again, not due to COVID), after a year of pseudo-pandemic worldwide there were about 2 million deaths attributed to COVID, i.e., the same number of annual tuberculosis deaths1🦶25... and this tuberculosis figure has always been there, and no one ever dreamed of shutting down the world for tuberculosis, despite this disease being more lethal than COVID.
In short, even with 2 million deaths worldwide in a year, assuming and not granted they are due to COVID-19, would it be an extraordinary number, a pandemic-level number? Looking at Bill Gates’ 2018 simulation of the next pandemic, one wouldn’t think so:
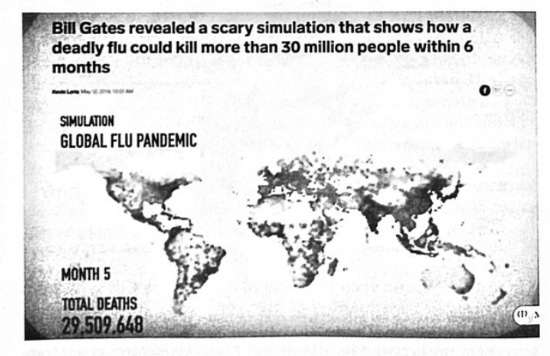
According to this pandemic simulation by Gates’ team, the next pandemic (the current one) should have caused nearly 30 million deaths in just 5 months! While it caused only 900,000 in 7 months!
Above all, what are the annual numbers of deaths worldwide from flu and respiratory diseases, the “area” in which COVID-19 falls? COVID is a respiratory pathology, inclusive of flu symptoms and pneumonias, both interstitial and thromboembolic, and what follows is the number of annual deaths worldwide from pneumonias and respiratory pathologies:
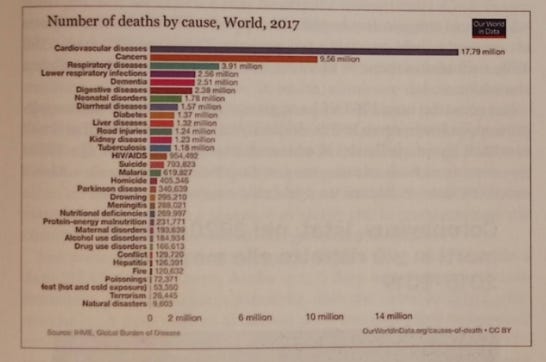
In 2017, the total deaths from respiratory diseases (pneumonias) and respiratory infections (flu and similar) was 3.91 million + 2.56 million = 6,470,000 deaths! If we also add tuberculosis, considered a respiratory pathology as well, we reach a total of 7,650,000!
Thus, even conceding as realistic the attribution of all two million COVID-19 deaths, we would still be at a fraction of deaths from respiratory causes. Unless it emerges that in 2020 total respiratory disease deaths rose to 10,000,000, one can only conclude that the usual respiratory deaths like flus and pneumonias were simply called by another name, COVID-19. And we are about to see that this is exactly what happened...
THE LATEST 2020 ISTAT DATA
The propaganda of the health dictatorship continues
January 2021
Last May I picked apart the ISTAT report claiming a 49% mortality increase in the period February 20–March 31, and showed it was more propaganda than real.
Over the months ISTAT has updated the data, up to the latest report published toward the end of December, picked up by all newspapers with headlines like that of Corriere Adriatico! Il Fatto Quotidiano had a similar headline, but specifying that the +84,000 deaths occurred between February and November 2020.
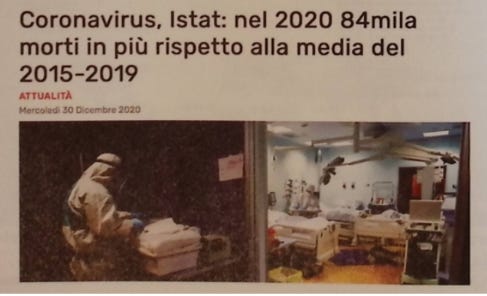
One immediately wonders why select the period February-November, and not the more logical January-November. Because ISTAT claims COVID started in February, and thus giving this number from February to November already pushes to link the mortality increase to COVID, something that, as we will see, ISTAT itself clarifies cannot be asserted. Anyway, it’s perfect for the media, to give large numbers immediately seemingly linked to COVID, thus passing the subliminal message that COVID caused an 84,000-death increase. But in reality it’s not so, and cannot be asserted, as we are about to see.
First, it must be stressed that, as usual, ISTAT goes out of its way to obscure or distort the real numbers. For instance, it presents a statistical comparison covering February to November, yet for 2020 alone it groups January and February together. This approach prevents independent verification — one is simply expected to take their word for it.
In fact, excluding January is illogical. Not only has it become widely acknowledged that the virus was already circulating by December 2019, but even ISTAT itself does not explicitly attribute the reported 84,000 excess deaths to COVID (except implicitly). These deaths could well stem from other causes, such as seasonal factors — especially since the cold season peaked in March 2020. Therefore, the most accurate comparison should include the entire January–November period of 2020.
Between January and November 2020, according to ISTAT data, there were 664,623 deaths in Italy. Yet even these figures are not fully comparable — nor entirely verifiable — since ISTAT itself admits that “the data on deaths in the second half of November cannot currently be considered fully consolidated.” Compared with the five-year average of roughly 583,396 deaths, 2020 shows an apparent increase of about 13.5%.
However, comparing a single year to a multi-year average tends to inflate the perceived significance of that year’s result. If we instead take 2017 as a reference point, the difference shrinks:
2020 — 664,623
2017 — 594,851
which equals an increase of approximately 11.7%.
The differential has lowered, and indeed one must recognize that there was an increase in mortality. Was it a truly unusual increase? It is a differential of 69,772 deaths.
For example, the mortality differential between 2014 (598,364) and 2015 (647,571) was 49,207 deaths, a difference of 8.2%, thus lower than the 2020-2017 differential, but not by so much.
If we then look at the differential between 2011 and 2017, a period when the population did not vary, the differential is 55,634, a 9.4% difference in favor of 2017. Here the difference with the 2020-2017 differential narrows even more, reducing to just 14,000 deaths, and 2.3%.
In short, 2020 could certainly set a death record (if November numbers are confirmed and December remains high), but these are still numbers not excessively above ordinary year-to-year mortality variations, certainly not such as to scream “terrible pandemic.” And in fact no definitive conclusion can be drawn until December deaths are available, which could lower the differential and bring it back into the range of differences between different years we just saw. Certainly in 2020 there was a higher-than-usual number of deaths, if as seems we exceed 700,000. In fact, ISTAT President Blangiardo immediately declared to the media that, given over 700,000 deaths, 2020 takes us back to World War II times:
As has been rightly noted, Blangiardo forgets to say, however, that in 1944 the Italian population was around 43 million, and thus for 2020 to be comparable to WWII deaths in 1944, with nearly 1/3 more population, 2020 should have had over 900,000 deaths! There, that mortality increase could have screamed possible, albeit still small, epidemic. Is it possible the ISTAT President doesn’t know these things? No, it’s not possible, but to maintain the fake pandemic news one must cling to anything.
On the other hand, to understand how this year is not so different from usual, just see what the same Blangiardo said in 2015 in an interview on Il Fatto Quotidiano:
“But let’s start from the origin of the mystery, demographer Gian Carlo Blangiardo’s analysis. From ISTAT data on the first seven months of 2015, Professor Blangiardo deduces a surplus of 39,000 deaths compared to the same period in 2014, ‘an 11% increase that, if confirmed annually, would bring 2015 deaths to 664,000 against 598,000 last year.’ A spike of 66,000 deaths (the estimate later revised to 68,000 with more recent data) that Blangiardo assimilates to those recorded only during the two world wars.”2🦶26
Thus, even in 2015 Blangiardo cried an 11% death increase, exactly the difference between the restricted February-November 2020 period and 2017, and as today, cried WWII! But no one thought then to scream “epochal pandemic”!
The truth is that, to speak of an epochal pandemic, as we saw above, 2020 should have at least 1 million deaths, compared to about 650,000 in recent years!
And even so it would be a small pandemic, considering the Spanish flu (with all doubts remaining on whether it was a viral pandemic) caused over 50 million deaths; and that, as we saw, Bill Gates in 2018 predicted the next pandemic capable of 30 million excess deaths in just 5 months!
To conclude this first part: there is no doubt that in 2020 something happened that slightly raised mortality; but it raised it to levels still within the possible variation delta, without any extraordinary leap, as one would expect from a true pandemic.
And above all, as Blangiardo himself says, we are not talking about COVID deaths, but about: “... overall deaths (thus not only those caused by COVID).”
Deaths from COVID?
In the period of January 30 to November 2020 there were 57,637 deaths attributed to COVID. The death increase in the same period would have been 83,985 deaths.
Obviously, all media jumped to assert and make believe that COVID contributed 68% (57,637 / 83,985). But even here, it is a purely propagandist maneuver, favoured by the general setup of the ISTAT Report, even if ISTAT itself, albeit in a way that doesn’t stand out too much, states that:
“It should be remembered, however, that the ratio between deaths reported to Integrated Surveillance and excess mortality in the February-November 2020 period cannot account for COVID-19’s actual contribution; this measure is indeed affected by methodological problems related to data consolidation (both Integrated Surveillance and Istat) and the difficulty in identifying deaths caused by COVID-19 when they occur in patients with numerous concomitant pathologies.”
In fact it is true that, according to ISS and the American CDC itself, in 96% of deaths with COVID there was an average age of 84 years and serious pre-existing pathologies, three in 63% of cases, two in 20% of cases and one in 13% of cases. But if this data were accepted, then one simply shouldn’t speak of COVID and pandemic at all.
Even if we accept the premise that all 57,000 recorded deaths were caused by COVID, they still cannot simply be counted among the 84,000 “excess deaths.” The reason is straightforward: such a claim would only be valid if COVID deaths were compared to those from respiratory and influenza-related diseases — the broader category to which COVID belongs. For instance, according to ISTAT data, in 2018 (the most recent year available) Italy reported 75,808 deaths from respiratory diseases.3🦶27
COVID deaths as of December 31 were calculated at about 74,000. The only way to verify COVID’s contribution to the mortality increase is to measure the increment brought by COVID to the total respiratory pathologies. If respiratory pathologies in total became about 150,000, then COVID’s contribution will have been total. But if total respiratory deaths remain around 75-80,000, then it will be evident that COVID was nothing but another name for the usual respiratory pathologies, pneumonias, flus, etc.
In fact, that this second hypothesis is likely is confirmed by various statistics on the near-disappearance of flu. For example, in the USA this is the comparative graph between flu cases in 2019 and 2020:
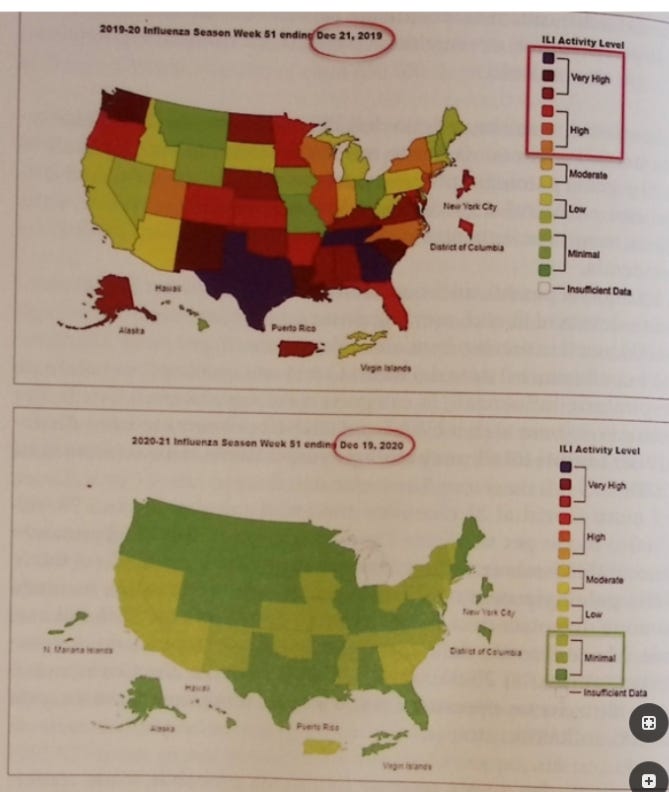
As seen from the previous graphs, we went from a High or Very High flu situation in 2019 to Minimal in 2020. And the same is happening in Italy. According to the Influnet report of December 12, 2020, in the week from November 30 to December 6, the flu circulation rate was 1.9 cases per thousand inhabitants, against 3 cases per thousand last season (from 174,000 to 115,000 cases); and in the latest bulletin the gap is even greater:
“In the 52nd week of 2020, the incidence of flu-like syndromes continues to be steadily below the baseline threshold with a value of 1.5 cases per thousand assisted. In the previous season in this same week the incidence level was 3.9 cases per thousand assisted.”4🦶28
Since data on causes of mortality are not published except long after, even over a year later, a serious statistical body would do better to remain silent and wait for that data.
ISTAT instead, while introducing caveats on the impossibility of assessing COVID’s contribution to excess mortality, attributes this impossibility to non-statistical reasons, and above all sets up its entire report on the continuous suggestion, more or less veiled, that the mortality increase is substantially linked to COVID. As we saw, from a statistical point of view, this is an assertion that cannot be made, and probably cannot be soundly made for at least another year.
But if it wasn’t COVID, what could have caused this undeniable—but not pandemic-justifying—increase in deaths?
Meanwhile, ISTAT states that “from late February to November, COVID-19 deaths represent 9.5% of total deaths.” In reality, this percentage is inflated: the correct figure is 57,637 ÷ 664,623 = 8.6%.
Excluding other possible considerations—which ISTAT does not address—the proportion of COVID-attributable deaths among the approximately 84,000 excess deaths is therefore 8.6%, corresponding to about 7,222 deaths. In other words, of the 83,985 excess deaths, only 7,222 can be attributed to COVID-19.
This means that the claim suggesting 57,000 COVID deaths account for over 60% of the mortality increase is unfounded. Of those 57,000 deaths “with COVID,” nearly 49,800 likely correspond to deaths that, in previous years, would have been classified as influenza or pneumonia. Consequently, the crucial question remains: what explains the remaining 76,763 excess deaths (83,985 – 7,222)?
I had already emphasized in my first analysis of the initial ISTAT report—and confirmed above with data from Bergamo and other cities—that the rise in mortality has largely been due to causes other than COVID-19. So, what really happened?
If we break down the data by periods, we find what ISTAT itself recognizes, namely that 2020 divides into three periods: the “first wave,” from February 20 to mid-May, where there was a fairly limited number of COVID positives but a high number of deaths; the intermediate phase, from mid-May to September, with very few cases and very few deaths; and then the aforementioned “second wave,” including October and November, where there was an explosion of positive cases, and also a substantial number of deaths with COVID, though fewer than in March. Let’s try to understand this dynamic well.
First, if we take the first seven months, we already see that the ratios change:
Period January-July
2020 - 426,289 deaths ÷ 2017 - 390,129 = +9.2%
We had seen how a 9.4% increase had already occurred in the comparison between 2011 and 2017. Thus, even if 2020’s mortality increase over 2017 leads to a mini-record, 2017 being a high-mortality year, the size of the increase remains within known parameters.
The important thing is to see how we went, in the 2020-2017 comparison, from a +9.2% differential in January-July to +11.7% in January-November: an increase of 2.5 percentage points.
To understand how this jump occurred with the alleged “pandemic wave,” let’s look at this ISTAT graph:
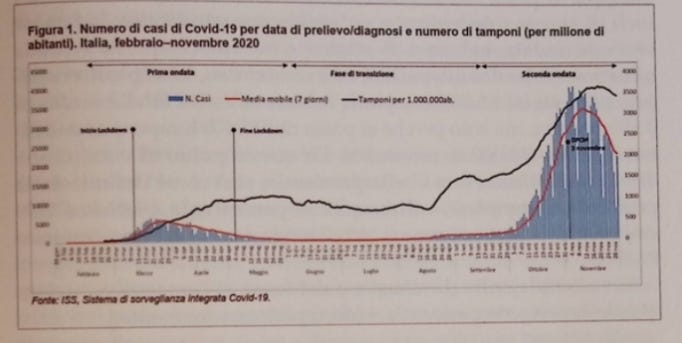
As can be seen, after the “first wave” (in quotes, because the very idea of “pandemic waves” is absurd), in which there were few positives (an average of 500 per day) against a small number of swabs (about 5,000 per day); there followed a phase where the number of swabs continued to increase, but the number of positives remained fixed near zero: despite about 10,000 swabs per day, in May-August positives continued to decrease. Interesting to note how only with the increase in swabs, which from September rose to 15-20,000 per day, the number of positives also starts to move, to begin a dizzying rise in both the number of swabs and positives starting in October and up to almost all of November.
In essence, this graph confirms that it is a PCR pandemic. As can be seen, the increase in cases is perfectly parallel to the increase in swabs. This is an important datum: if the pandemic had truly risen in October and November, there should have been an increased ratio between cases and swabs, i.e., a higher percentage of positive cases for the same number of swabs. In concrete terms: in September, an average of 15,000 swabs were performed per day, producing about 1,500 positive cases. Since this graph is presented to justify the transition from a phase of pandemic cessation, in the months of June to September, to a pandemic explosion, the famous second wave, in October and November, this second wave should have led to, say, 3,500 positives still on the same 15,000 swabs. Instead, we do reach an average of 3,500 positives, but only because we go from 15,000 swabs in September to over 40,000 in November. From this point of view, one can say the opposite, namely that the pandemic, as defined by swab positivity, decreased in percentage, because if 1,500 cases out of 15,000 swabs are 10%, 3,500 cases out of 40,000 swabs are 8.75%.
Despite this decrease in the contagion rate—and thus of the alleged pandemic—deaths still increased:
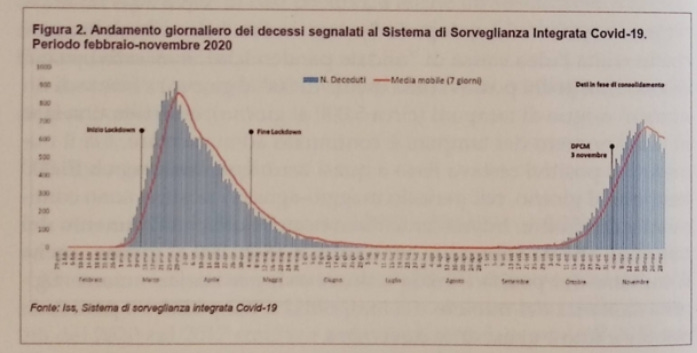
How is it possible that, with the decrease in contagiousness, there is such a radical increase in deaths? To better understand the relevance of this datum, we must compare the period of the first wave with that of the second.
In March, at the supposed peak of contagion, Italy recorded about 800–900 deaths per day, yet the number of positive cases was only around 500–600. In other words, there were even more deaths attributed to COVID than confirmed positive cases — an absurd disparity that reflected what we denounced from the start: countless deaths were labeled as “COVID” without any verified positive swab, many of which were unreliable to begin with.
By contrast, in November, at the height of the so-called second wave, the daily toll stood at roughly 600–700 deaths — but this time against as many as 3,500 positives. The supposed lethality of SARS-CoV-2 therefore plummeted from over 100% to just 18.5%.
This dramatic collapse alone should have marked the official end of the “pandemic.” It clearly showed that, even assuming the virus existed as claimed, its alleged danger had diminished enormously. Yet, since this simple and statistically undeniable fact contradicts the dominant narrative, officials and media avoided any discussion of lethality. Instead, they kept repeating that November’s death numbers were “similar to March’s,” while ignoring that only a fraction of those deaths were truly attributable to COVID-19. In fact, between October and November, out of 134,737 total deaths, only 21,162 — about 15% — were linked to COVID.
This is a higher percentage than the annual average (9.5%), but still minimal compared to the total number of deaths. And if the low percentage of COVID on total deaths in March could even be justified with the excuse that not enough swabs were being done, this certainly cannot be said of October and November, where the number of swabs rose to 40,000 per day. Unfortunately for the pandemic narrative, this near-tenfold increase in swabs produced a strange mix of exponential increase in positives together with, oh horror, a reduction in the number of deaths compared to March! If we compare the March-April period, the peak of the first wave (February contributed only the last week and with a little over 1,000 deceased with COVID), and the October-November period, where the second wave allegedly exploded, we see that:
COVID positives went from 207,794 in March-April to 1,329,324 in October-November (an increase of nearly 700%);
total deaths went from 157,879 in March-April to 134,767 in October-November, a 15% reduction!
COVID deaths went from about 30,000 in March-April to 21,162 in October-November, a 30% reduction!
What kind of pandemic is it where the infected multiply sevenfold and deaths, both total and with COVID, decrease?
ISTAT’s reply to this evident contradiction is that from March to October we learned to treat COVID, and thus despite the explosion of positives there are fewer deaths. But this justification doesn’t hold, because treatment protocols are exactly the same as in March and April, attempts to introduce new treatments like hydroxychloroquine were rejected, and home therapy protocols with drugs, which should have reduced hospital crowding, were presented by health authorities only on November 14, and have not yet been implemented, thus having no impact on the October-November period.5🦶29
And if it were true that the decrease in deaths despite the explosion of positives was due to the fact that we now know how to treat COVID, it is unclear why we must submit to the restrictions imposed on us, from more or less stringent lockdowns, to bans on gatherings, to masks, even mandatory all the time at school, or to vaccines!
The truth is that the second wave was, even more evidently than the first, a pandemic of swabs, of asymptomatic positives, who have now been established as neither infectious nor able to be contagious. In a previous article of mine, I reported a COVID swab certificate that was “honest”:
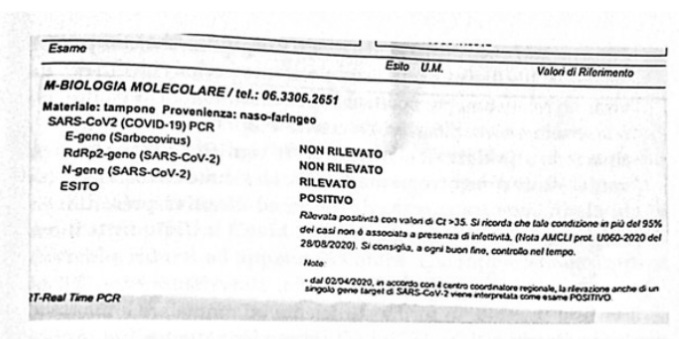
In this honest certificate it is clearly stated that, since the positivity result was obtained with more than 35 PCR cycles, “... such condition, in more than 95% of cases, is not associated with the presence of infectivity.”
As I urged at the time: why is this truth known to all not taken into consideration by politicians? After all, now even the WHO has taken a clear position on this. Let’s see the first WHO statement:
“The probability that a person who tests positive (SARS-CoV-2 detected) is actually infected with SARS-CoV-2 decreases as positivity rates decrease, net of test specificity. Therefore, health workers are encouraged to consider test results together with clinical signs and symptoms, confirmed contacts, etc.”
This is a strong statement, because if the swab is in itself insufficient to establish actual COVID positivity without the support of “clinical signs and symptoms,” it is already evident that 90% of positives, who are asymptomatic, cannot be declared either infected or infectious. Already for this reason alone, all the numbers on positives sold to us in 2020 should be discarded, thus realizing that there was no pandemic. The WHO continues:
“The constructive principle of RT-PCR means that with patients with high levels of circulating virus (viral load), relatively few cycles will be needed to detect the virus and therefore the Ct value will be low. Conversely, when samples report a high Ct value, this means that many cycles were required to find the virus. In some circumstances, the distinction between background noise and actual virus presence is difficult to establish.”6🦶30
Despite the obvious expressive caution, the truth emerges clearly: if the virus is present in a sufficient form to make one sick and infect, few PCR cycles will be needed; if the virus is detected with too many cycles, it is very difficult to establish that it is not mere background noise. Here the position is clear-cut: it is not only that a result with over 30-35 cycles indicates a low viral load and thus non-infectious, but precisely that at this Ct level (PCR cycles), the results even detect not necessarily the virus but “background noise,” which has nothing to do with the virus. As we will see in the chapter on swabs, a series of important articles, and established PCR science, have established that the maximum PCR cycle level (Ct) for which a case can be considered positive is 20-25. We will see how at 30 Ct there is over 80% false positives, and at 34-35 Ct up to 100% false positives.
With the number of cycles normally used in Italy, generally above 35, and in the vast majority of cases above 40 and up to 60 cycles, the number of declared positives who are actually such collapses to 0%. Thus, even the huge numbers of positives in October and November reported by ISTAT, all obtained with PCR swabs performed with over 35 cycles, should be reduced to zero!
But with this true number they could not have screamed about the explosion of the second wave, and could not have continued their devastating lockdowns.
At this point, even the deaths attributed to COVID would have decreased, since all attributions of deaths to COVID were based on the positivity of the deceased, before or after death, to the PCR swab. This means that, to be generous, the number of deaths attributable to COVID in October and November, instead of 21,162, should be reduced to just 635 deaths, which represent just 0.47% of total deaths.
Even if one stubbornly insists on counting asymptomatic positives as “COVID cases,” we must still ask: what caused the actual mortality increase—modest as it was and hardly “pandemic”-level—given it clearly wasn’t due to COVID? After all, on an excess of 70,000 deaths, COVID accounts for just 9.5% per the ISTAT COVID-to-total deaths ratio (or 8.6%, as previously noted). And indeed, aware of the problem, ISTAT throws in a scarcely plausible explanation that somehow continues to link the mortality increase to COVID:
“Excess mortality was estimated by comparing, for the same period, 2020 data with the average deaths of the previous five-year period (2015-2019). In this way, it is implicitly assumed that the spread of the epidemic produces an increase in the frequency of deaths even not directly referable to COVID-19 surveillance, i.e., to the number of positive deceased cases.”
That is, as if the 2 million swabs performed were not enough, nor the numerous cases of deaths attributed to COVID without even a COVID swab performed (fake as it is worth), now ISTAT also wants to insinuate that even the excess deaths not referable to COVID are actually somehow linked to COVID. Well, I would say that in part this is possible, because COVID was above all a political-economic coup d’état, with the imposition of lockdowns and other devastating socio-economic limitations, and it is known that unemployment increase linked to lockdowns produces deaths. Indeed, another blow to ISTAT’s credibility is its insistence that lockdowns reduced road accident mortality, completely silencing what is known to science:
“Job loss causes extreme suffering. Every 1% increase in the unemployment rate increases the probability of drug overdose deaths by 3.3% and suicides by 0.99%, according to data from the National Bureau of Economic Research and the medical journal Lancet... Add then the predictable deaths from alcohol abuse caused by unemployment. Health economist Michael French from the University of Miami found a significant link between job loss and excessive alcohol use—even up to full-blown alcoholism.... The impact of layoffs goes beyond suicides, drug overdoses, and alcoholism anyway. In general, an unemployed person’s mortality rate is 63% higher than that of an employed person, according to data from the Journal Social Science & Medicine.”7🦶31
Sure, they can tell us they imposed hiring freezes and distributed redundancy pay. But this doesn’t apply to all small entrepreneurs and self-employed who haven’t been able to work for almost a year, and who in the best case received less than €1,000 total.
🦶25 Gengenbacher M & Kaufmann S.H.E., Mycobacterium tuberculosis: success through dormancy, FEMS Microbiol Rev 36 (2012) 514-532
🦶30 WHO, WHO Information Notice for IVD Users, https://www.who.int/news/item/14-12-2020-who-information-notice-for-ivd-users In reality, following this link one will not find the cited texts, because in the meantime WHO has deleted the original document replacing it with a more “moderate” and ambiguous one, though the substance doesn’t change much.
I think what they did was draw suspicion to all scientific research and the numbers involved. Numbers can be jigged to prove anything. So not only is the research suspect, so are the scientists and the people who reported the results. This is what happens when you play with the truth.
Leslie
I watched a couple of videos of this man who explained how our body's defences work and how difficult it would be for this mRNA platform to do what they said it could. He looked quite healthy, too, so hearing of his death is surprising. Thank you for translating these chapters. I have read economic stuff which says banks were, yet again, in a crisis, so Covid was rolled out to funnel money to the banks. Also, pHarma in big trouble as patents ending resulting in loss of revenues, so something had to be conjured to make money.