

Chapter 3 - Apandemia - Part 3
By Stefano Scoglio - translated to English from Italian

Here is part 3 of Chapter 3 from the book Apandemia, written by Stefano Scoglio. This chapter appears to have been previously released on Facebook. But of course, links to Facebook do not work well because, as we all know, Facebook is a criminal enterprise. I personally do not use it often, as it is so very corrupt.
The book is also listed on Amazon, where it has 62 reviews and a 4.7-star rating. One reviewer wrote: “Serious researcher. They should include it among the textbooks in schools throughout that entire part of the world that was deceived with the fear of the virus.”1
THE EUROMOMO GRAPH
As confirmation that there was no increase in mortality due to a pandemic—and thus no pandemic—the European agency EuroMomo, which records mortality across the continent, published the following map on July 31, 2020:
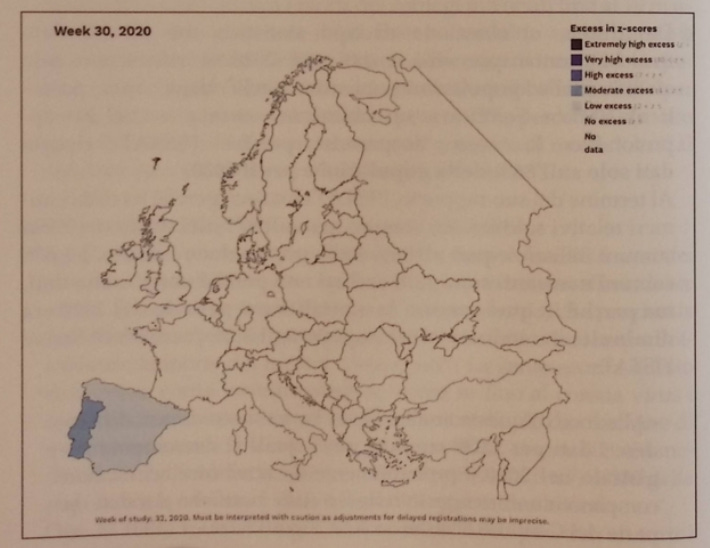
As seen in the choropleth map2, across almost the entire continent, except for a slight increase in Spain and Portugal, there was no excess mortality. In subsequent months, perhaps sharply reprimanded by European politicians, EuroMomo tried to remedy the error of telling the truth and continues to publish statistics titled “Increase in Mortality,” headlines that prove entirely unfounded when examined in detail.
But the choropleth map was published, and it confirms the thesis that there was no increase in mortality—and thus no pandemic—as shown by my analysis of the ISTAT Report on mortality. But then, if there is no pandemic causing deaths, why are we continuing to do lockdowns and extend the state of emergency? Thanks to the invention of the new pathology of “asymptomaticity”: just test positive on a COVID-19 swab and you’re considered sick, and to this is added outright manipulation of COVID-19 mortality data.
MANIPULATION OF COVID-19 TESTS AS THE ENGINE OF THE PERPETUAL PANDEMIC
Saturday, July 25, 2020
We will examine in more detail—in a subsequent chapter and from both technical-scientific and legal viewpoints—how the indefinite extension of the pandemic rested on the definition of the new pathology of asymptomaticity. At the base of this program lies the use of completely unreliable swab tests, which the EU itself defined as invalid (never authorized or validated). But today, I want to emphasize a maneuver of clear, conscious data manipulation—and COVID case definition criteria so absurd they surpass the barrier of the ridiculous (if it weren’t tragic). This maneuver was developed by the American CDC.
What is happening in the USA has now become central for Italy as well. In Italy, it is now difficult to find deaths classified as COVID-19, or even a decent number of infected people. Here, the government justifies its attempts to extend the emergency and lockdown (perhaps only partial) through appeals to the international situation. Thus, Minister Speranza (”Corriere della Sera”, July 21, 2020) states:
“The international situation worries me greatly, we are at the worst moment of the epidemic in the world, this situation does not allow us to say that it is a thing of the past. It will be a thing of the past only when we have a vaccine.”
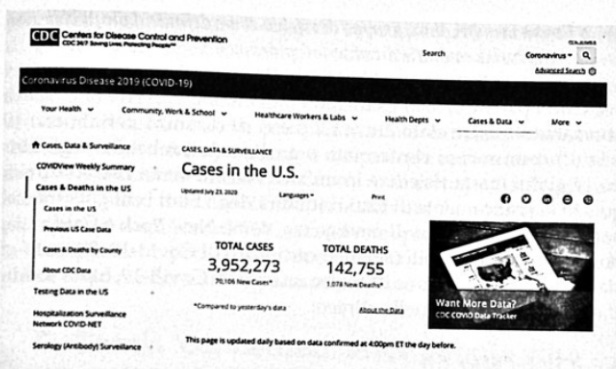
The reference is mainly to the US situation, where every day tens of thousands of cases of asymptomatic infected are reported, given enormous weight by the regime media, despite deaths being fewer and fewer and ICU wards emptier and emptier. Thus, even today the CDC (the US health institute, until a few days ago directly responsible for counting COVID deaths and infected) reports as many as 70,000 new infected in a single day.
In fact, it is a very high number of infected, and Trump dismissed it saying it’s due to doing many more swabs than before. This is true, but only in part: it’s true that with fake swabs you get huge numbers of false positives, but here there’s a more specific element of malice and manipulation concerning the new COVID definition introduced by the CDC last April, circulated in May, which produced its first results starting in June up to the current explosion. If you look closely, even in the document shown above, it doesn’t speak of “positives” for COVID-19, but of cases. Yes, because under the CDC’s new definition, for a case to be defined as COVID-19 you don’t even need to test positive on the swab test; it’s enough that the case is “probable”.
(https://www.cdc.gov/ndc/conditions/coronavirus-disease-2019-covid-19/casedefinition/2020/4/) The link doesn’t work, maybe it was this one: https://ndc.services.cdc.gov/case-definitions/coronavirus-disease-2019-2020-08-05/
And how is a “probable” case defined?
“A case is probable if it meets clinical criteria AND epidemiologic evidence, without confirmatory laboratory testing for COVID-19.”
That is, for a case to be probable—and thus count as a full COVID case—it’s enough to have epidemiologic evidence and clinical [evidence]. These two parameters are defined by the CDC as follows:
Epidemiologic Linkage:
One or more of the following exposures in the 14 days prior to symptom onset:
Close contact with a confirmed or probable COVID-19 case; OR
Close contact with a person with a clinically compatible illness and linkage to a confirmed COVID-19 case.
Travel or residence in an area with sustained and current community transmission of SARS-CoV-2.
Being a member of a risk group as defined by public health authorities during an outbreak.
Thus, for the epidemiologic element to exist, beyond close contact (having been within 2 meters distance for at least 10 minutes) with a confirmed or even just probable case in the last 14 days, it’s enough to reside in an area considered at COVID risk: this practically makes all citizens of states whose governors have declared a state of emergency, like New York and California, potential probable (and thus certified) COVID-19 cases. And for full certification as a COVID-19 case, it’s enough to meet the other criterion, the clinical one:
Clinical Criteria:
At least two of the following symptoms: fever (measured or perceived), chills, rigors, aches, headache, sore throat, new loss of taste or smell
At least one of the following symptoms: cough, shortness of breath, or difficulty breathing
A severe respiratory illness with at least one of the following:
Clinical or radiographic evidence of pneumonia
Acute respiratory distress syndrome (ARDS).
And no alternative diagnosis more likely.
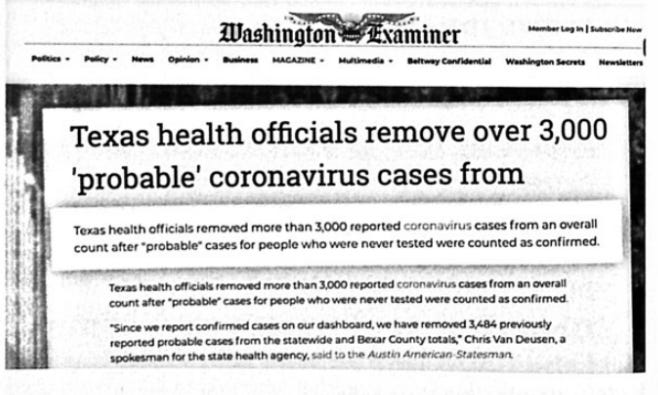
Thus, for the clinical criterion to be met it’s enough to have two symptoms among fever (even subjectively perceived), chills, rigors, aches (myalgias), headache, sore throat, new disorders of smell and taste; or just one symptom among cough, shortness of breath, or breathing difficulties. In short, if you live in a state whose governor has declared a state of emergency, and you have a headache along with tremors, or aches and joint stiffness, or even just a cough, you immediately become a “probable” COVID case, meaning you are immediately counted as a COVID case. And since, once a COVID case is established, all those who have been in contact with the subject are automatically suspected of COVID to be tested or checked for symptoms like cough, or headache + aches, it’s evident how the number of COVID cases can rise rapidly. And it’s also thanks to this that there has been the explosion of COVID cases which, even if asymptomatic, serve to maintain the rhetoric of the pandemic and the still-imminent danger that thus requires further lockdowns. At a certain point, Trump realized these CDC tricks and decided that data should no longer be reported by states to the CDC, but to a specific committee at the White House. And a few days after this move, the first corrections to the crazy numbers disseminated by the CDC arrived:
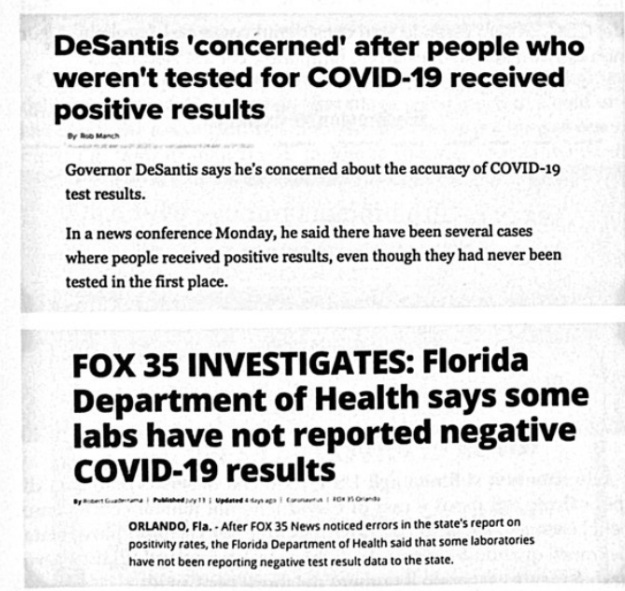
Here we see how, after journalists investigated and found that some labs were not reporting negative tests and always giving 100% positivity rates, it emerged that the positivity rate, instead of 98%, was just 9.4%! A big difference, which can hardly result from an accidental error, and can only be the fruit of outright fraud on the numbers. Things weren’t much different in Texas either: Texas health officials removed as many as 3,824 deaths attributed to COVID-19 under CDC criteria, i.e., having been considered “probable” cases without ever being tested with swabs or serological tests.
And the issue doesn’t stop at the USA, since the same problem of hyper-counting COVID deaths and cases (which we Italians know well) has also emerged in the UK, where they stopped the daily count of deaths when it emerged that Public Health England (PHE) had greatly exaggerated the number of COVID deaths:

As the Center for Evidence-Based Medicine at the University of Oxford itself pointed out, PHE counted as COVID deaths even those who had recovered, been discharged, and then perhaps died later of heart attack or car accident. This mania for counting even car accident deaths as COVID deaths seems very widespread, if it’s true that even in Florida a young man killed in a motorcycle accident was reported as dead from COVID:
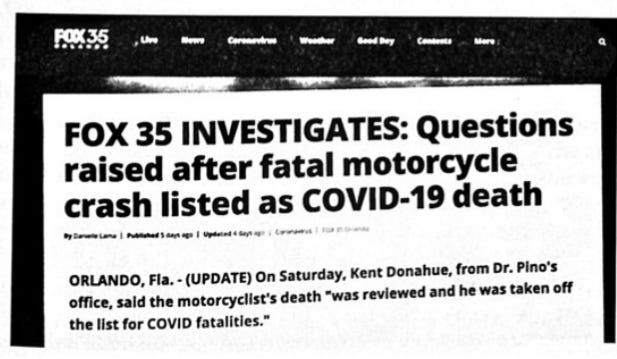
The journalist even reports that the doctor responsible for the case told him that in his opinion the car accident may actually have been caused by COVID-19!!!
I recall how these falsifications are common in Italy too. I myself made a post on FB (https://www.facebook.com/ScoglioStefano NOTE: link does not work…post from June 15) where I reported two cases of over-80s who died from end-stage cancer, classified as COVID-19 without even being swabbed, and taken from the family with no possibility of autopsy... and in the comments on the post, both on my page and profile, there are at least another 50 testimonies of similar cases!
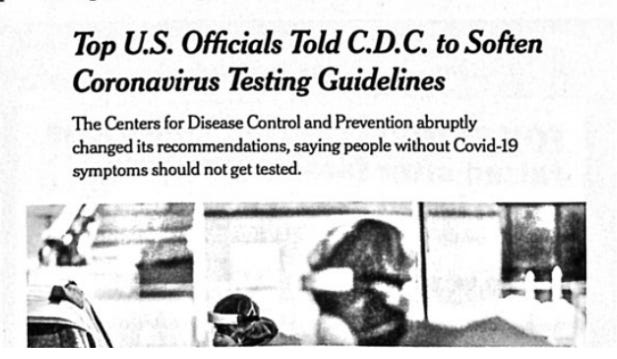
To conclude this contribution of mine centered on the epidemiology of the false pandemic, coming to the latest available numbers. Let’s start by saying that the biggest change happened precisely in the USA, thanks to Trump. The US President decided to take control of the US Deep State health structures, FDA and CDC, and imposed new criteria on them for calculating COVID-19 and its mortality. First, under pressure from the President, the CDC changed its policy on COVID tests, and now recommends doing swab tests only on individuals with clear COVID-19 symptoms, thus eliminating the buffoonery of seeking out as many asymptomatics as possible and passing them off as dangerously contagious sick people:
Unfortunately, with the approaching US elections, the practice of inflating the number of deaths resumed unabated, because the Democrats and Deep State knew that only by maintaining the idea of a serious pandemic could they push for mail-in voting, to carry out the biggest electoral fraud in history. But for a while, it seemed the pseudo-pandemic had its days numbered.
Even Italian TV news, after weeks of bombarding us every day with alarmist news on the number of US infected, rather than saying that very few infected remain, decided to avoid talking about COVID-19 in the USA altogether. This must also have been contributed to by the latest American CDC document, which re-evaluated all deaths with COVID-19, doing what the Italian Istituto Superiore di Sanità had done, i.e., removing from the death count all those who had serious concomitant or pre-existing pathologies:
“In 6% of deaths, COVID-19 was the only cause of death listed. For deaths with conditions in addition to COVID-19, on average there were 2.6 additional conditions or causes of death.”🦶note 223
It must have been hard for the CDC, the main engine of the pandemic along with the WHO, to have to admit that 94% of deaths attributed to COVID-19 are actually attributable to other pathologies, mostly at least three other pathologies. This recalls the data from the Italian Istituto Superiore di Sanità, which specified that only a minimal percentage of deaths had no other serious pathologies, and that even in the latest version of its analysis, confirms a datum even more radical than that of the American CDC:
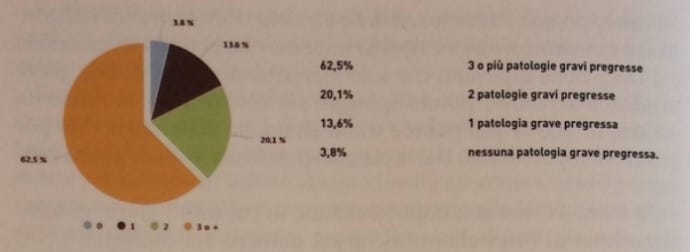
In other words, only 3.8% of deaths recorded as COVID would be truly attributable to COVID itself . To this is added the data on the average age of deaths WITH COVID-19:
“The average age of deceased patients positive for SARS-CoV-2 is 80 years (median 82, range 0-109, InterQuartile Range - IQR 74-88).”🦶note 234
In the USA the average age was even set at 84 years, and since life expectancy in the 1940s (the birth period of our 80-year-olds) was 60-65 years🦶note 245, deaths at 80-84 years had already lived 15-20 years beyond their life expectancy (and even 30 years more in the case of the numerous over-90s who died), which cannot be irrelevant in evaluating mortality incidence.
This too confirms there was no pandemic at all. Whatever happened with COVID-19, we can say its essence was much ado about nothing...
https://www.amazon.ca/Apandemia-scienza-grande-truffa-storia/dp/B09LGWWRX4#averageCustomerReviewsAnchor
A choropleth map is a type of thematic map where each geographic area (such as a country, region, or county) is shaded or colored according to the value of a specific variable, like population density or mortality rate.
🦶note 22 CDC, Weekly Updates by Select Demographic and Geographic Characteristics, Provisional Death Counts for Coronavirus Disease 2019 (COVID-19), September 2.
🦶note 23 Epicentro, Istituto Superiore di Sanità, Caratteristiche dei pazienti deceduti positivi all’infezione da SARS-CoV-2 in Italia, September 2020: https://www.epicentro.iss.it/coronavirus/sars-cov-2-decessi-italia?fbclid=IwAR3e0LxSBIi9_LsSwgcrTt6P1zEt3hljEHw-VYtrU_5v9RBMxXr3wBCxQxPM#l
🦶note 24 Mastroianni F., Come è cambiata l’aspettativa di vita nel mondo, 16 Nov 2017, Il Sole 24 Ore; The 1940 Census, at: https://www.uslearning.net/1940-census.html
You have to wonder how much Davos was involved with this extraordinary denial of our human rights. I recently saw Simon Schama's take on the Holocaust, 80 years on, on PBS. His warning was this happens little by little than all of a sudden. In Canada medical doctors spoke out on their practical experience of the"apandemic". They were silenced and threatened to have their licence taken away from them if the contradicted the government narrative. A lot of grooming going on to prepare us for a total authoritarian takeover.
Leslie
“A case is probable if it meets clinical criteria AND epidemiologic evidence, without confirmatory laboratory testing for COVID-19.”
On and on.
https://www.thescottishsun.co.uk/news/scottish-news/6027823/coronavirus-scotland-jason-leitch-test-rubbish/