

Urgent Need for Closer Examination
the elephant in the room

This post originates from an interview between Wilson Sy, author of Excess Deaths in the United Kingdom: Midazolam and Euthanasia in the COVID-19 Pandemic1, and Maajid Nawaz, host of Radical Media – by Maajid Nawaz, published on Substack on February 22, 2024. I will refer to this interview in future posts.
If not for short attention spans this article would be longer

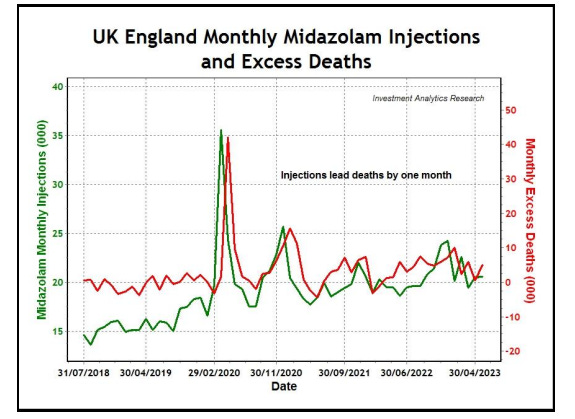
Maajid Nawaz notes that in 2024, the UK faces a 10–20% excess mortality rate, a global trend observed in countries with COVID-19 mandates. Wilson Sy’s paper, finds a correlation between midazolam injections and excess deaths from April 2020 through July 2023, with a stronger statistical signal (90% coefficient in 2020, 59% in 2021–2023, p-value 0.0007) than any link to SARS-CoV-2 or COVID-19 vaccinations. The interview also discusses the NHS’s NG163 protocol, which guides midazolam use in end-of-life care for terminally ill patients, raising concerns about its application.
Summary of NICE NG163 Guideline:
The NICE COVID-19 guideline (NG163), published April 3, 2020, recommends midazolam for severe breathlessness in end-of-life care, often off-label, with doses of 2.5–5 mg subcutaneously every 2–4 hours or 10–60 mg over 24 hours via syringe driver. While the NICE NG163 guideline emphasizes informed consent from patients and families before using midazolam in end-of-life situations, it allows clinical flexibility as a non-mandatory recommendation. In 2020, despite the underutilization of hospitals (72% occupancy vs. 90%+) and idle Nightingale facilities, unnecessary countermeasures and panic likely hindered seeking informed consent.
The Scottish COVID-19 Inquiry suggests that consent for midazolam was often absent. Carol Ann Currie, Principal Carer at Randolph Hill Nursing Home, testified on March 26, 2024, that “nine times out of ten, regardless of what the resident’s symptoms were, they were prescribed just-in-case medication”2 (end-of-life drugs like midazolam and morphine), emphasizing concerns about overuse.
Video was taken and edited from this post by biologyphenom

Sy’s analysis identifies a correlation between midazolam use and excess deaths, stating:
“Importantly, excess deaths remained elevated following mass vaccination in 2021, but were statistically uncorrelated to COVID vaccination, while remaining significantly correlated to Midazolam injections. The widespread and persistent use of Midazolam in UK suggests a possible policy of systemic euthanasia. Unlike Australia, where assessing the statistical impact of COVID vaccination on excess deaths is relatively straightforward, UK excess deaths were closely associated with the use of Midazolam and other medical intervention. The iatrogenic pandemic in the UK was caused by euthanasia deaths from Midazolam and also, likely caused by COVID vaccination, but their relative impacts are difficult to measure from the data, due to causal proximity of euthanasia. ”
Policies like NG163 appear to have contributed to the deaths of vulnerable populations, resembling historically eugenics-like practices associated with Nazi Germany, and closer examination is warranted, while notable that there is very little examination taking place at this time as the subject receives very little attention as anyone who discusses this subject is hidden by computer algorithms.
The assertion that the SARS-CoV-2 virus was largely absent in early 2020 is supported by several observations. Official reports, such as the UK Health Security Agency’s statement on March 19, 2020, downgrading COVID-19 from a “high consequence infectious disease,” suggested a lower-than-expected threat.3 Case numbers remained far below projections, with the anticipated million cases not materializing. Hospitals reportedly remained underutilized, with elderly patients discharged to care homes in anticipation of a surge that never occurred. Consequently, Nightingale hospitals stood largely unused, prompting discussions about their closure.4 These indicators suggest the SARS-CoV-2 virus was not as prevalent as had been projected by institutions and pundits who were boosted by algorithms online.
If you don't want to see my posts subscribe or follow 🤣
Excess Deaths in the United Kingdom: Midazolam and Euthanasia in the COVID-19
Pandemichttps://www.medclinrese.org/open-access/excess-deaths-in-the-united-kingdom-midazolam-and-euthanasia-in-the-covid19-pandemic.pdf
Guidance High consequence infectious diseases (HCID) https://www.gov.uk/guidance/high-consequence-infectious-diseases-hcid
Hospital bed capacity and usage across secondary healthcare providers in England during the first wave of the COVID-19 pandemic: a descriptive analysishttps://bmjopen.bmj.com/content/11/1/e042945
''If not for short attention spans this article would be longer.'' - Too funny even though i condensed hours long testimonies into minutes some people have said they are still too long.
''If you don't want to see my posts subscribe or follow''- LOL I'm going with ''like, share and comment if you don't care'' just so you know that's taken okies?
Being more serious. I've been dumbfounded by the lack of people making their own Scottish COVID inquiry clips after i point stuff out and that somehow i have to be the world spokesperson as a non awake medic, no reputation on the line layperson.
''Policies like NG163 appear to have contributed to the deaths of vulnerable populations, resembling historically eugenics-like practices associated with Nazi Germany.''
Fact check. TRUE
In Anna’s statement we see another comment on COVID protocols being similar to the Nazi eugenics program of the 1930’s.
https://biologyphenom.substack.com/p/scottish-covid-19-inquiry-impact-554?utm_source=publication-search